Chronic central
serous chorioretinopathy (CSC) is a well-recognized entity characterized by
accumulation of serous sub retinal fluid (SRF) which induces a localized
detachment of the neurosensory retina. Patients can present with various visual
complaints including central scotoma, metamorphopsia and micropsia. It is most
frequently unilateral and affects young adult males more commonly. There is
often a history of recent stress and the subject usually has a type A
personality. The visual deterioration in chronic cases results from damage to
the underlying retinal pigment epithelium (RPE) and photoreceptors. The
underlying pathogenesis involves multifocal areas of choroidal vascular hyper
permeability1,2. It is speculated that the fundamental mode of
action of photodynamic therapy (PDT) with verteporfin (Visudyne; Novartis
Pharma AG, Switzerland) utilized for the treatment of CSC is the shutdown of
the vessels in the choriocapillaris resulting in hypo-perfusion and extended
remodeling of choroidal vasculature. We approached this case of chronic
symptomatic CSC by treating him with half-fluence rate (25 J/cm2),
without modifying the dose of verteporfin (6 mg/m2). The
choice of a suitable fluence rate enables one to evade indirect damage to
surrounding structures such as RPE atrophy, ischemia of the choroid, and
development of secondary choroidal neovascularization (CNV) because of less
choriocapillaris damage3. The intervention was done after seeking
permission from the hospital’s ethical and research committee. The author has no
financial interest in the products used. The authors
declare no conflict of interest.
CASE REPORT
We report a case of 49 years old male,
shopkeeper by profession, who was suffering from right sided recurrent chronic
CSCR. (Figure 1,2) His condition dated back to 2002. He was treated with
various treatment modalities including oral acetazolamide and also received multiple
intravitreal injections of Anti VEGF. Argon laser was also applied but the CSCR
never resolved.
The earliest available OCT (done in October
2012) shows right sided CSCR involving the fovea with central macular thickness
of 631 microns in the right eye (Figure 3).
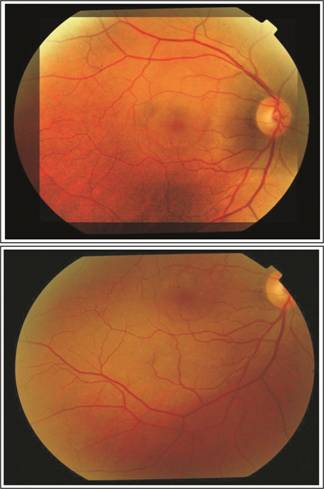
Fig. 1: Color fundus photograph of Right eye showing the dome shaped
elevation of central serous chorioretinopathy.
We decided to treat him with half-fluence
PDT in June 2015. At that time, his vision was 6/36 in the right eye and
central macular thickness of 483 microns (Figure 4). The PDT was done on 10th
of June 2015 to the right eye.
It was decided to treat him with half-fluence
PDT (25 J/cm2) instead of the regular 50 J/cm2). The half-fluence rate was
chosen as it is sufficiently effective while at the same time reducing the
collateral choroidal hypo perfusion and thus being safer as demonstrated in the
“Visudyne in Minimally Classic Choroidal Neovascularization Study Group study”.
After the treatment the
patient was instructed to avoid strong light and wear protective glasses for 48
hours. We followed him with 2 monthly serial OCT scans which showed gradual
resolution over a period of 6 months. (Figure. 5) His latest OCT scan performed
on 5th January 2016 showed complete resolution of the sub-retinal
fluid in the right eye with central macular thickness of 190 microns. At this
time his visual acuity was 6/9 OD (Figure 6).
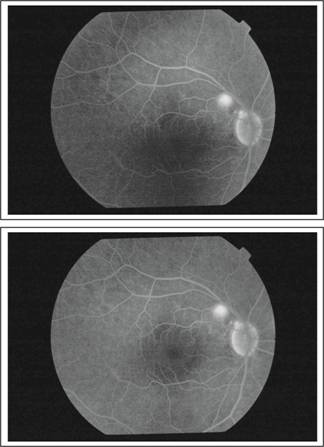
Fig. 2: FFA of the same eye localizing the area of leakage.
The patient did not
experience any adverse systemic event neither during Verteporfin infusion nor
in the follow-up period. No collateral damage of the retina was observed for
instance the growth of CNV or detachment of the pigment epithelium.

Fig. 3: OCT Macula OD October 2012.
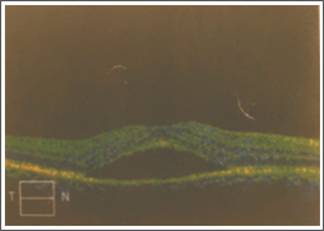
Fig. 4: OCT Macula OD June 2015 (OCT on the day of treatment).

Fig. 5: OCT Macula OD October 2015 (3 months after treatment).

Fig. 6: OCT Macula OD January 2016 showing complete resolution of the
sub-retinal fluid 6 months after half-dose PDT.
DISCUSSION
In this case, we used half-fluence rate (25
J/cm2) and routine quantity of verteporfin (6mg/m2) to increase the
effectiveness and at the same time decrease the associated damage caused by PDT
in a patient with chronic CSCR. We observed a steady decrease in the central
macular thickness from the initial 483 microns to 190 microns and simultaneous
gain in visual acuity from 6/60 to 6/9 at the last follow-up visit (Fig. 4-6).
Currently there is no
definitive therapy available for cases of either acute or chronic CSCR. Diverse
efforts have been made at devising a therapy for this condition including Argon
laser to seal off the leakage points4,5. Although treatment with
laser may considerably reduce the span of the ailment, it has not been found to
influence the final visual acuity or rate of recurrence of CSCR6.
Smretschnig et al have reported very good outcomes in visual acuity and
significant decrease in the central foveal thickness using half-fluence PDT in
cases of both acute and chronic CSCR7. The largest study conducted
so far was by Chan et al which included 48 eyes with a follow-up of one year
and revealed the complete absorption of SRF in 95%of eyes with betterment in
visual acuity compared to a control group8.
Reibaldi et al have
assessed low-fluence PDT (25J/cm2) as opposed to standard fluence
(50J/cm2) and found that the best-corrected visual acuity improved
at 12 months in both the groups with resolution of SRF in a considerable number
of eyes. However, they also noted substantial choriocapillaris non-perfusion in
44% of cases which were treated with standard fluence PDT versus 0% in those
which underwent treatment with half-fluence PDT9. Shin et al have
also stated identical findings10.
CONCLUSION
Central serous
chorioretinopathy is a challenging clinical problem. The use of reduced fluence
PDT appears to be a safe and potent treatment modality for chronic CSCR.
Author’s
Affiliation
Dr. Qasim
Lateef Ch
FCPS,
FRCS, FCPS (VR)
Associate
Professor of ophthalmology
Eye
Department Jinnah Hospital/
Allama
Iqbal Medical College, Lahore.
Dr. Tehmina
Jahangir
FCPS, Fellowship in vitreoretina
Assistant
Professor of ophthalmology
Eye
Department Jinnah Hospital/
Allama Iqbal Medical College, Lahore.
Role of
Authors
Dr. Qasim
Lateef Ch
Case
diagnosis, treatment and follow-up
Dr.
Tehmina Jahangir
Case
diagnosis, documentation, treatment, literature search and discussion writing.
REFERENCES
1.
Rosenthal JM and Flaxel CJ. Half-dose and half-fluence photodynamic therapy for central
serous chorioretinopathy. J Eye Ophthalmol. 2014; 1: 2.
2.
Rouvas A, Stavrakas P, Theodossiadis PG, Stamatiou P, Milia M,
Giannakaki E and Datseris I.
Long-term results of half-fluence photodynamic therapy for chronic central
serous chorioretinopathy. Eur J Ophthalmol. 2012; 22: 417-22.
3.
Shinojima A, Kawamura A, Mori R, Fujita K and Yuzawa M. Detection of morphologic alterations by spectral-domain optical
coherence tomography before and after half-dose verteporfin photodynamic
therapy in chronic central serous chorioretinopathy. Retina. 2011; 31: 1912-20.
4.
Silva RM, Ruiz-Moreno JM, Gomez-Ulla F, Montero JA, Gregorio T,
Cachulo ML, Pires IA, Cunha-Vaz JG and Murta JN. Photodynamic therapy for chronic central serous
chorioretinopathy: a 4-year follow-up study. Retina, 2013; 33: 309-15.
5.
Ruiz-Moreno JM, Lugo FL, Armada F, Silva R, Montero JA, Arevalo
JF, Arias L and Gomez-Ulla F.
Photodynamic therapy for chronic central serous chorioretinopathy. Acta Ophthalmol.
2010; 88: 371-6.
6.
Nicolo M, Zoli D, Musolino M and Traverso CE. Association between the efficacy of half-dose photodynamic
therapy with indocyanine green angiography and optical coherence tomography
findings in the treatment of central serous chorioretinopathy. Am J Ophthalmol.
2012; 153: 474-480.
7.
Smretschnig E, Ansari-Shahrezaei S, Hagen S, Glittenberg C, Krebs
I and Binder S. Half-fluence
photodynamic therapy in chronic central serous chorioretinopathy. Retina, 2013;
33: 316-23.
8.
Chan WM, Lai TY, Lai RY, Tang EW, Liu DT and Lam DS. Safety enhanced photodynamic therapy for chronic central serous
chorioretinopathy: one-year results of a prospective study. Retina, 2008; 28: 85-93.
9.
Reibaldi M, Boscia F, Avitabile T, Uva MG, Russo A, Zagari M, Occhipinti
F, Russo V, Reibaldi A and Longo A. Functional retinal changes measured by microperimetry in
standard-fluence vs. low-fluence photodynamic therapy in chronic central serous
chorioretinopathy. Am J Ophthalmol. 2011; 151: 953-960.
10.
Shin JY, Woo SJ, Yu HG and Park KH. Comparison of efficacy and safety between
half-chorioretinopathy. Retina, 2011; 31: 119-26.